

Healthcare in Madagascar – The Critical Gaps
Since relocating to the beautiful island of Ile Sainte Marie (Nosy Boraha) and founding NORA-Madagascar seven months ago, I’ve gone through the expected period of adjustment, navigating the minor coughs and colds that come with a new environment and new microbes. However, a recent and debilitating crisis – a persistent, raging fever that struck me down—was a brutal awakening and my first real experience with healthcare in Madagascar.
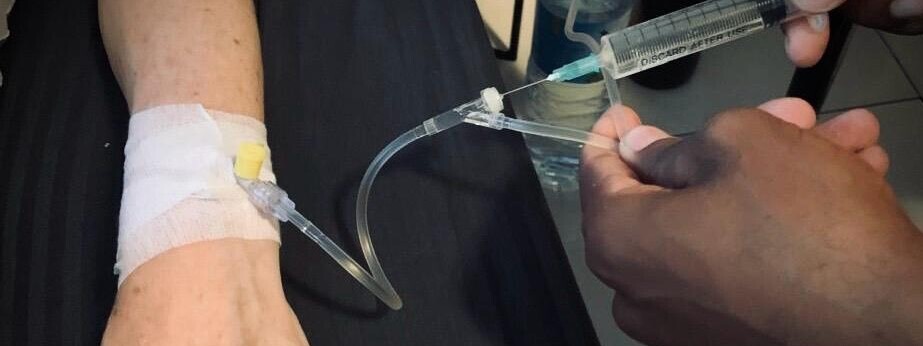
This experience became a stark reminder of the immense privilege of private health insurance. When my illness escalated, the local public hospital’s acute lack of funding, staff, and basic equipment was immediately apparent. My path to recovery required a private doctor making house calls, administering IV fluids, and ultimately, a flight to the capital, Antananarivo, for necessary diagnostics. For the local population, this private intervention is an impossible fantasy. This level of care – being able to travel to get treatment, specialized doctors, high-level diagnostics – is a lifeline for expats and the wealthy, but it highlights a painful truth: for the majority of the Malagasy population, this lifeline simply does not exist.
The Malagasy Healthcare Crisis: An Overview
The public health system in Madagascar faces deep, systemic challenges that translate into a severe lack of Universal Health Coverage (UHC). These issues are especially magnified in rural and remote areas like small islands and the deep countryside.
- 🏥 Critical Lack of Infrastructure: Many primary health facilities (CSB – Centre de Santé de Base) are poorly maintained, lack electricity for consistent nighttime care or vaccine storage, and often have insufficient basic equipment.
- 💰 Financial Barriers: The Cost of Care: With a significant portion of the population living in poverty, the high cost of consultation, medicine, and transport becomes an immediate barrier. Health expenditure per capita is among the lowest in the world. People often delay or forgo essential treatment, viewing hospitals as a last resort.
- 🗺️ Geographic Isolation and Accessibility: For up to 30-40% of the population, walking over 5 to 10 kilometers to the nearest health center is the norm. This physical obstacle, compounded by a poor road network, makes emergency care impossible and routine care difficult, particularly for mothers and children.
- 💊 Drug and Staff Shortages: Public facilities frequently suffer from a shortage of essential medicines and qualified medical personnel. In some regions, there are as few as 0.20 doctors per 1,000 patients, placing immense strain on the limited staff who are available.
- 🦠 High Burden of Disease: The country contends with high rates of preventable infectious diseases, including malaria, diarrheal diseases, and lower respiratory tract infections. Malnutrition rates, especially among children, are also alarmingly high, exacerbating disease vulnerability.
The Two-Tiered System: A Matter of Life and Death
My personal story perfectly illustrates the devastating reality of a two-tiered healthcare system:
The Private Track: For those with means and insurance (like myself), quality treatment, specialized diagnostics (scans, tests), and immediate care are available, often in the capital city, ensuring survival and recovery. This resembles the availability of private hospitals common even in wealthier nations like those in Europe, where private care offers speed and comfort.
The Public Track: For the vast majority of local communities, the consequences are literal matters of life and death. Care is delayed, limited, or inaccessible due to distance, cost, and poor-quality facilities. Crucially, even public hospitals and emergency rooms often demand immediate payment for essential services, medicine, or supplies (the “no money, no treatment” reality). This is a critical distinction from systems where public care is guaranteed at the point of need. This disparity leads to drastically higher mortality rates and sustained health crises, particularly in maternal and child health.
The difference between these two tracks is not just a matter of comfort or convenience; it is the difference between surviving a medical crisis and succumbing to a preventable illness.
A Path Forward: The Role of NGOs and Global Partners
The efforts of NGOs and international partners are vital in bridging this gap. Organizations like UNICEF, MSF (Doctors Without Borders), PIVOT, GFF and others are actively working on the ground to:
- Strengthen primary health infrastructure
- Support community health workers in remote villages.
- Provide mobile clinics and essential medications.
- Combat malnutrition and major diseases like malaria.
These initiatives and the collective efforts of the international community, are essential steps toward achieving true Universal Health Coverage in Madagascar.
We must shift the focus from a system that relies on luck and wealth to one that provides equitable, quality care for every Malagasy citizen, regardless of where they live.
Luck and Privilege
My experience on Ile Sainte Marie – a successful recovery – was a story of luck and privilege, not universal provision.
The existence of private hospitals in developed countries offers a premium service, but the public alternative is typically a functional safety net that guarantees care for all. In Madagascar, however, the public health system’s financial barriers and lack of resources mean that for millions, the difference between the “private track” and the “public track” is literally the difference between living and dying from preventable or treatable conditions. When a public emergency room demands payment before treatment, the system has failed the principle of basic human dignity.
🤝 A Call to Action: Investing in the Lifeline
Bridging this chasm requires targeted investment in the most vulnerable parts of the system. Efforts are underway by the Ministry of Health, the GFF, UNICEF, PIVOT, and other partners to:
- Eliminate Financial Barriers: Pilot programs that remove or subsidize fees for essential care, especially for mothers and children.
- Strengthen the Frontlines: Invest in training and deploying Community Health Workers (CHWs) – the true healthcare lifeline for the 40% of the population geographically isolated from a clinic.
- Bolster Essential Infrastructure: Equip Basic Health Centers (CSBs) with supplies, electricity (for vaccine cold chains), and medicines.
You can dive deeper into the facts here:
World Health Organization (WHO) data indicates that Madagascar has a severe lack of healthcare personnel, noting a ratio of approximately 1 doctor for every 11,000 people (or 0.17 per 1,000 population). Madagascar – Country Disease Outlook (See page 1, “Limited access to healthcare”)
Significant Geographic Barriers to Access: A large percentage of the population lives far from basic health facilities, making timely care difficult or impossible. Healthcare Access and Poverty Reduction: SEED’s Impact in Rural Madagascar (Notes “nearly half of the population living more than 5 km from local health centres”) and Geographic barriers to establishing a successful hospital referral system in rural Madagascar (Notes “more than half lived over 4 hours away” from a hospital)
Critically Low Health Expenditure: The country’s total health expenditure as a percentage of its Gross Domestic Product (GDP) is extremely low, reflecting a severe lack of public investment.Current Health Expenditure (CHE) in Madagascar is among the lowest globally, recently reported as low as 3.25% of GDP in 2022 (a decline from 3.5% in 2021). Madagascar Health spending as percent of GDP (World Bank data via TheGlobalEconomy.com)
Poor Maternal and Child Health Outcomes: The Maternal Mortality Ratio (MMR) is dangerously high, with estimates around 445 deaths per 100,000 live births (2023 data). Madagascar | World Bank Gender Data Portal (See “Maternal mortality ratio”)
UNICEF data also shows a high under-five mortality rate (e.g., 65 deaths per 1,000 live births in 2021/2022). Madagascar (MDG) – Demographics, Health & Infant Mortality (See “Under-five mortality rate”)

